Dalberg uses cookies and related technologies to improve the way the site functions. A cookie is a text file that is stored on your device. We use these text files for functionality such as to analyze our traffic or to personalize content. You can easily control how we use cookies on your device by adjusting the settings below, and you may also change those settings at any time by visiting our privacy policy page.

Smallholder farmers – which number over half a million in Kenya alone – are among the most underserved group by financial and information services. Investment in this sector is hampered by lack of understanding and visibility into what, exactly, smallholder farmers need and want. Yet growth in agriculture is at least twice as effective in reducing poverty as growth in other sectors. There is a clear opportunity to match need with services.
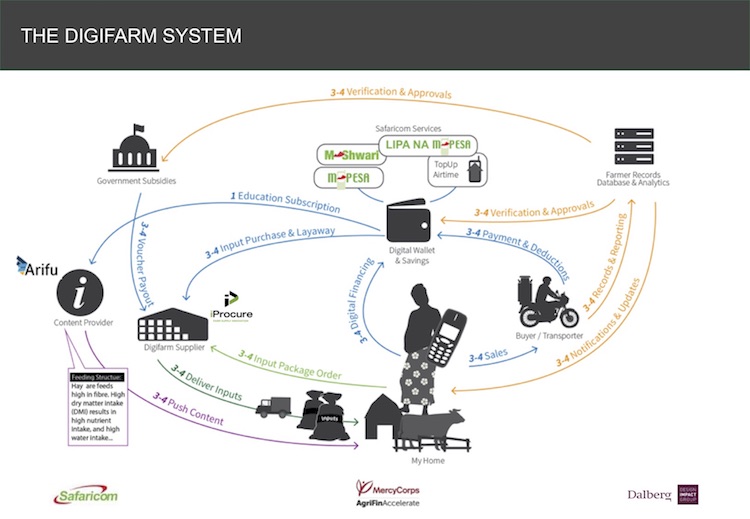
Enter DigiFarm. DigiFarm allows farmers to buy discounted inputs, receive farming advice and access loans from their 2G phones in either English or Swahili. It launched in Kenya in March 2017 and has reached over 800,000 farmers to date. The platform recently won a Fast Company 2018 World Changing Idea Award and Safaricom’s parent company, Vodafone, is looking to replicate DigiFarm in other markets including Egypt, Tanzania, and India.
To create DigiFarm it was essential to understand Kenyan smallholder farmers’ practices and challenges. Dalberg supported the Mercy Corps’ AFA program and DigiFarm partners (led by Safaricom) in DigiFarm’s creation. The Dalberg team worked to understand the needs and behaviors of smallholder farmers, develop a minimum viable product, identify and provide strategy support for partner service-providers that complement Safaricom’s offering to meet farmers’ needs. Dalberg worked to pilot and support multiple rounds of evolution and scale-up of the DigiFarm platform.